
Complete blood cell count
Introducción
Hello, welcome to this 4th class of the Hematology course provided by the University of Guanajuato. In this class we are going to review some aspects about the complete blood cell count.
The complete blood cell count or hemogram Is one of the most requested laboratory tests. It is divided into three main groups: Red blood cells or erythrocytes, White blood cells or leukocytes, Thrombocytes or platelets. The basic measurements that a hemogram contemplates are:
- Number of erythrocytes. They are measured in cells per microliter (cells/ml) of blood.
- Number of leukocytes. Its unit is also cells/ml.
- Platelet count. It is recorded in units per microliter of blood (u/ml).
- Hemoglobin (Hb) concentration. It is measured in grams per deciliter (g/dL).
- Hematocrit value. It is counted as a percentage (%). Ratio of erythrocyte volume to total blood volume.
- As well as the erythrocytes Indices:
- Mean corpuscular volume (MCV). Indicates the average size of red blood cells, expressed in femtoliters (fl).
- Mean corpuscular hemoglobin (MCH). The amount of hemoglobin per red blood cell and is given in picograms per cell (pg/cell).
- Mean corpuscular hemoglobin concentration (MCHC). It reveals the amount of hemoglobin relative to cell size (hemoglobin concentration), in grams per deciliter (g/dL).
It is important to consider aspects of the preanalytical stage because some parameters could be affected if some errors are made. Differences between the manual and automated process are going to be revised, as well as some cellular alterations present in peripheral blood smears.
Desarrollo del tema
The complete blood cell count Is a very useful and easy to perform laboratory examination. Many hematologic diseases and malignancies can be detected with this simple study. As previously mentioned, It Is divided in the study of three main groups: red and white cells, and platelets.
The pre-analytical stage aspects must be taken into account In the following conditions:
- Fasting: 8 hours Is recommended, since hemoglobin levels are altered with lipemic sera. Infants should not fast more than 4 hours.
- Fluids: dehydration makes it difficult to draw blood, drink moderate amounts of water before a blood test should be recommended to the patients. Hemoconcentration may result with dehydration as well.
- Exercise: 24 hours prior to blood collection, do not perform intense physical activity (erythrocyte variation).
- Alcohol: Do not consume alcoholic beverages the night before the study (changes in liver enzymes, glucose).
- Tobacco. Hypoxia state: transient erythrocythemia.
- Menstrual period: false anemia (hematocrit decrease)
- Medications: Oral contraceptives, antibiotics, certain vitamins, corticosteroids, aspirin (platelets).
- Mild illness (cold or flu, for example) is better to delay the test at least three weeks.
- It is not advisable to schedule a blood draw if in the previous 72 hours the patient has undergone diagnostic studies that may alter the results, such as an intravenous contrast test.
- Stress. It is important to avoid stress and stay relaxed before and after the blood test.
Measurement parameters
Hemoglobin
It is the main component of erythrocytes. It is a conjugated protein that serves as a vehicle for the transport of oxygen (O2) and carbon dioxide (CO2). One molecule consists of two pairs of polypeptide chains (globin) and four heme prosthetic groups, each containing one atom of ferrous ion. Each heme group is precisely located in a gap or fold of each of the polypeptide chains.

Types of hemoglobin

Hemoglobin derivatives
Oxyhemoglobin: Hb bound to oxygen.
Carbaminohemoglobin: Hb bound to CO2.
Hemiglobin (methemoglobin [Hi]) Hi: a derivative of hemoglobin in which ferrous iron is oxidized to the ferric state, resulting in the inability of Hi to combine reversibly with oxygen. The polypeptide chains are not altered.
Sulphohemoglobin: A mixture of partially oxidized denatured forms formed during oxidative hemolysis. During oxidation of hemoglobin, sulfur from some source is incorporated into the heme rings of hemoglobin, giving rise to a green hemochrome. The new oxidation usually results in denaturation and precipitation of the hemoglobin as Heinz bodies. Sulphohemoglobin cannot carry oxygen but can combine with carbon monoxide to form carboxysulphohemoglobin. Unlike methemoglobin, sulphohemoglobin cannot revert to hemoglobin, and remains in cells until they break down.
Carboxyhemoglobin (HbCO)
Endogenous CO: produced by degradation of heme to bilirubin (0.5%) from carboxyhemoglobin in the blood and is increased in hemolytic anemia.
CO + Hb = 210 times more affinity.
HbCO cannot bind or carry oxygen = anoxia
MANUAL DETERMINATION OF HEMOGLOBIN CONCENTRATION
Cyanomethemoglobin cyanmethemoglobin (hemiglobin cyanide, HiCN)
Blood is diluted in a solution of potassium ferrocyanide and potassium cyanide.
The potassium ferrocyanide oxidizes the iron in hemoglobin to form hemiglobin (Hi; methemoglobin) and the potassium cyanide converts cyanide ions to the HiCN form, a color-stable compound whose absorption maximum is at 540 nm.
– Drabkin’s reagent –
Increases in absorbability not due to hemoglobin may be caused by turbidity due to abnormal plasma proteins, hyperlipidemia.
Large number of leukocytes or fat droplet; any of these causes can produce an increase in light scattering and apparent absorbance.
Other methods
Sodium lauryl sulfate
Sodium lauryl sulfate is a surfactant that lyses red blood cells and forms a complex with the released hemoglobin. This complex is stable for a few hours and shows a maximum absorbance peak at 539 nm peak absorbance at 539 nm. It is used in automated analyzers, but the complex is unstable in the long term.
Azide-MetHb
This method is based on the conversion of hemoglobin into the stable product azide-MetHb, which has an absorbance spectrum almost identical to cyano-MetHb, using in this case a less toxic reagent. The results are comparable with the cyano-MetHb method, being a good alternative as a manual method. Its use in automated analyzers is not recommended due to the explosive potential of sodium azide.
Cooximetry
It is based on a spectrophotometric technique, in which hemoglobin and its fractions present absorbance peaks at specific wavelengths and thus have a characteristic spectrum that follows the Lambert-Beer law.
After hemolyzing the blood sample by physical or chemical agents to release the hemoglobin from the red blood cells, the results of the measured absorbances at multiple wavelengths are used by software to calculate the concentration of each hemoglobin derivative (O2 Hb, HHb, COHb, MetHb, SHb). The absorption range is 520-620 nm.
The ctHb is calculated through the sum of the derivatives.

Errors in hemoglobinometry
Errors inherent to the sample
Incorrect venipuncture technique: hemoconcentration.
Errors inherent to the method
HiCN, method of choice, except for SHb.
Errors inherent to the equipment
Pipetting, uneven cuvettes, wavelength adjustment, filters.
Operator errors
Fatigue, patience and criticality. Use of automated equipment.
Manual hematocrit
Ratio of the volume of erythrocytes to that of whole blood.
Expressed as a percentage (conventional) or as a decimal fraction (SIU).
Heparin and EDTA.
Macro and micro methods, or indirectly as the product of mean corpuscular volume by erythrocyte count (automated equipment).
Blood at room temperature: erythrocyte inflation between 6 and 24 hours increases Hto and MCV.
Micro method
Capillary hematocrit tube about 7cm long with a uniform hole of about 1mm.
Fill the tube to at least 5cm. Seal the empty end. Centrifuge in the radial recesses of the hematocrit centrifuge head with the sealed end away from the center (10 000 to 12 000 rpm).


Interpretation of results
Adult males: 41 to 51 %
Females: 36 to 45 %
Value below: anemia
Value above: polycythemia

Causes of error
Centrifugation.
Duration and speed.
Sample.
Position, muscle activity, stasis due to maintained tourniquet.
Excess EDTA, Hb and cell counts are not affected.
Other.
Failure to mix blood properly, inappropriate reading of cell and plasma level, inclusion of leukocyte stratum as part of erythrocyte volume.
Macrohematocrit
Wintrobe tube
Mix the blood, take sample with Pasteur pipette, fill the Wintrobe tube, centrifuge at 3000 rpm for 30 minutes, read the value on the scale of the tube.

Manual erythrocyte count
Blood cell counting chamber, hemocytometer, Neubauer chamber.
Glass microchamber excavated in a special slide and closed by a coverslip.
Allows dilution of blood cells and their subsequent visualization under a microscope.
Dilutor pipettes
There are two types depending on the erythrocyte or leukocyte count. The design of both is similar and consists of a properly calibrated capillary with an ampullary dilatation or bulb at its proximal end, so that the volume that can contain this dilatation is always an integer multiple of that corresponding to the capillary itself.
Leukocytes: dilution 1/20
Erythrocytes: dilution 1/200

Cells counting chambers (hemocytometer)
Thick glass slide (3 mm thick), one of its surfaces has three parallel prisms sculpted on it, of which the central one is divided into two identical hemi prisms separated by a transverse groove, which allows two different samples to be placed simultaneously without mixing with each other.

PROCEDURE:

The most commonly used reticule model is the Neubauer model, consisting of 9 large squares, each with a surface area of 1 mm2. The four corner squares are used to count leukocytes, and the central square, which has a greater number of reference lines, is used to count erythrocytes and platelets.

Blue circles correspond to leukocyte counting zone. Red circles correspond to erythrocyte counting zone.
DIFFERENTIAL LEUKOCYTE COUNT.

Counting technique
1. Place the smear on the microscope stage. Observe at 100X
2. Count 100 leukocytes following the counting scheme. Note the respective number of neutrophils, eosinophils, basophils, lymphocytes and monocytes.

Leukocyte Reference Values

Suggestions to differentiate them:
Does it contain cytoplasmic granules?
Determine the color of the granules if possible.
Examine the nucleus of the cells for shape and density. Use RBCs as a measure

Using the nucleus as a criterion:
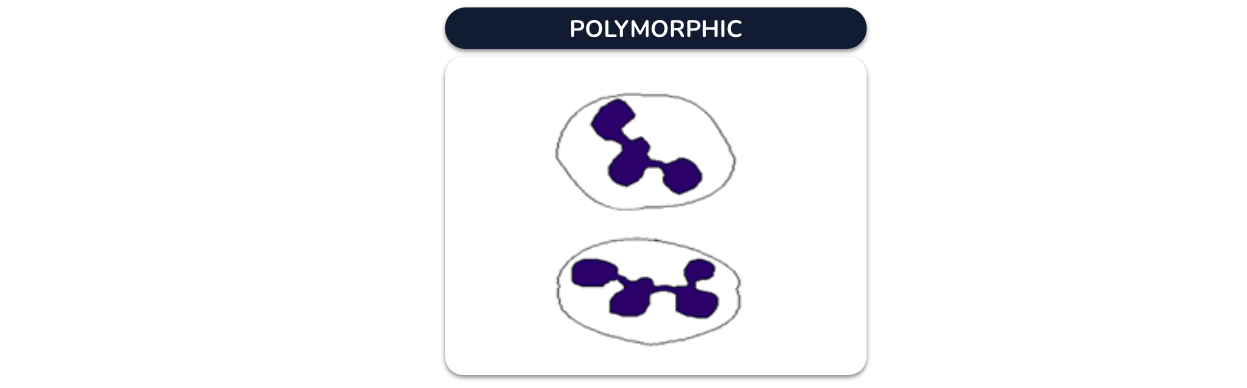
Neutrophils: A highly variable nucleus with more than two lobes. Small bridges connect the lobules. Typically dense, staining dark, dark blue or almost black.
Basophills and eosinophils have a nucleus with two distinct lobes connected by a narrow band of nuclear material. They are dense, but stain less darkly than neutrophills. These nuclei are usually «hidden» behind cytoplasmic granules.

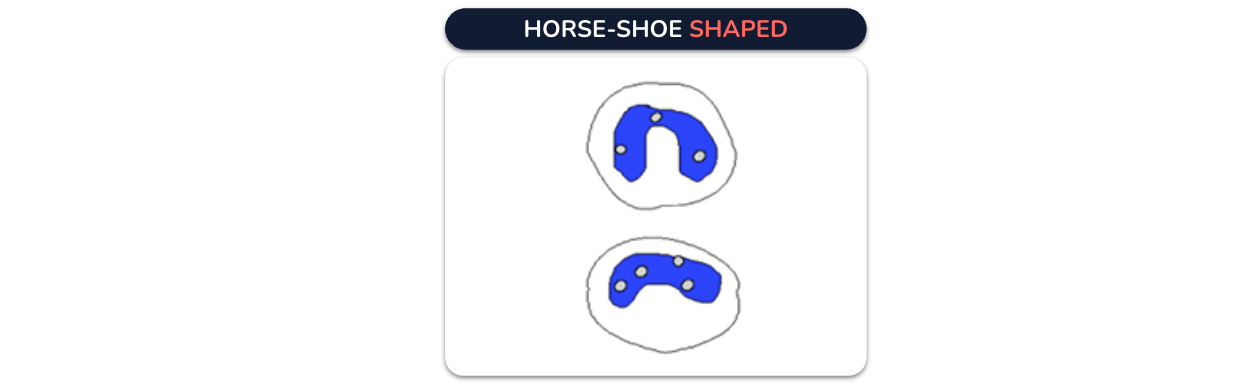
Monocytes contain a nucleus with circular or irregular vesicles of a lighter shade. They are horseshoe-shaped although it is not always very evident if not observed at a proper angle. They are the least dense of the leukocytes, staining a lighter shade of blue.
Lymphocytes have a characteristic nucleus that occupies most of the cell volume. They are dense, staining so dark that they almost appear black.

Automated blood cytometry
Wallace Coulter (1949) developed a particle counter based on the change that particles produce when passing individually through an orifice or opening that separates two media with different electrical potential (principle of electrical resistance or impedance).
Since 1980, automated continuous flow analyzers have incorporated the measurement of laser light scattering at two different angles, becoming flow cytometers whose complexity and performance have been evolving.
The intersection of each cell with the light causes the emission of a series of light signals that, when properly analyzed, make it possible to differentiate many of their properties (size, granulations, structural complexity, characteristics of the nucleus, among others) or their behavior when they encounter certain markers.

Fundamental
The measurement of concentration is usually carried out simultaneously with that of volume.
Variations exerted by cells when they pass through an electromagnetic field.
Three methodologies: impedance, light scattering and fluorescence (combined form).
Impedance: cell volume
Light scattering: leukocyte subpopulations.
Fluorescence: immunophenotypic analysis of leukocytes, cell viability, intracellular RNA quantification (reticulocytes).
Features
Hydrodynamic approach. Prevents cells from passing through the edge of the aperture hole or backing up and interfering with the reading of other cells.
Aperture hole diameter. Determined by the analyzer itself according to the cells in question. Permeability.
Current intensity. Continuous and sensitive, not excessive because it damages the cells.
Dilution of the cells. Coincidence error or counting defect when several cells pass through the opening hole at the same time. Very high cell concentration (alarm, dilution and retest).
Impedance
Resistance offered by cells to the passage of electric current when passing through an aperture hole separating two media with different potentials.
Change in electrical resistance (impulse).
The pulses generated are directly proportional to the size of the cell (cell volume) and the number of cells passing through the aperture hole per unit time is proportional to their concentration in the electrolyte medium.

Numeral data
Quantitative representation (SIU)
Histograms
Bi parametric graphical representations of a numerical variable. Frequency distribution graph (height).
Cytograms
Multiparametric representations
Most useful for differential leukocyte count.
Erythrocyte histogram
The erythrocyte volume is recorded, up to 250 fL. Normal erythrocytes have a volume of 80 to 100 fL. The gray lines show the differences in 50 fL intervals. Histograms should fall within the green lines and begin and end at the baseline (x-axis). With microcytic erythrocytes, the entire curve will shift to the left. With large erythrocytes, it will shift to the right.

In almost all analyzers, it is possible to superimpose the normal distribution to be able to answer whether the erythrocytes are microcytic or macrocytic. The normal curve corresponds to the one marked with the thickest blue line.
From the histograms, the parameters RDW-SD and RDW-CV can be calculated, which makes it possible to evaluate the distribution of red cells without the need for a blood smear.
RDW: Red Cell Distribution Width; ADE, Amplitude of Erythrocyte Distribution.
Histogram interpretation
The histogram will NOT directly reflect the cell count but will reflect the volumetric distribution of the erythrocytes.
Parameters derived from histograms:
MCV: mean corpuscular volume, by direct measurement of the arithmetic average of the volume of all erythrocytes included in the sampling.
RDW (Red Cell Distribution Width): mathematical measurement of histogram width. Greater or lesser degree of anisocytosis in the sampled erythrocytes. Measure of the deviation of the red cell volume.

Platelets
Higher than normal number: thrombocytosis, formation of blood clots that can cause a stroke.
Lower than normal number may result in extensive bleeding.
In some cases, inducing a lower platelet number may be possible, for example, if a person has had heart surgery.
The platelet number can be lowered by a daily intake of acetylsalicylic acid or other drugs that help reduce it.
Counting is performed at the erythrocyte opening, particles between 2 and 20 fL are counted as platelets. Particles such as bubbles or powder can be superimposed at the lower end. Microcyte erythrocytes can be introduced at the upper end.

Hemolysis: the counter can count erythrocyte fragments as platelets, it should be suspected when the curve does not end.


Light scattering
Analysis of the effect on a beam of high-intensity monochromatic light (laser) exerted by blood cells as they cross each other, one by one, in their trajectory.
Helium-neon
Argon-krypton
Helium-cadmium
Each time a cell gets in the way of the laser beam, there is an interruption of the photon passage or shadow that is cast on a dark field detector and a scattering of the beam itself that is diffracted:
- Diffracted (changes direction due to the effect of the cell surface),
- Refracted (changes speed due to the effect of the cellular structures)
- Reflected (reverses direction due to the effect of the opaque structures).


Absolute vs relative account
The relative count corresponds to the percentage of cells obtained from a differential count.
Absolute count: leukocyte count x 1000 x % specific cells expressed in decimal (lymphocytes, neutrophils, etc.).
WBC = 2.5 x 103/mL
% Lymphs = 30%.
Absolute lymph count = (2.5) (1000) (0.3) = 750 lymphs/mL
WBC = 8.3 x 103/mL
Neutrophil % = 50%
Absolute neutrophil count (ANC) = (8.3) (1000) (0.5) = 4150 neut/mL
In order to make a correct assessment, both values must be considered. For example, a relative neutrophil value of 70% could be within normal values; however, if the total WBC count is 20 000, the absolute value (20x1000x0.7) would be an abnormal value of 14 000.

Leukocytosis: WBC above 10 000
Neutrophilia
Lymphocytosis
Eosinophilia
Monocytosis
Basophilia
An increase in all five types of leukocytes is rare; when it occurs, it is usually due to dehydration and hemoconcentration.
Leukopenia: WBC below 4000



Patients with severe leukopenias should be protected from anything that alters the integrity of the skin, which may put them at risk for an infection that they will not be able to fight off.
They should not be subjected to intramuscular injections, rectal temperatures or enemas.
- Some drugs that can cause leukopenia:
- Antimetabolites
- Barbiturates
- Antibiotics
- Anticonvulsants
- Antithyroid drugs
- Arsenic
- Antineoplastics
- Cardiovascular
- Diuretics
- NSAIDS
- Heavy metal poisoning
Patients with WBC less than 500 are at risk for fatal infection.
Reticulocyte counts ETICULOCYTE COUNTS
They can be counted using a flow cytometer and are based on the amount of light absorbed by aggregated and stained organelles of the reticulocytes.
The results are recorded as the number of reticulocytes (%) of the total number of erythrocytes.
They can also be counted in a hemocytometer using a microscope.
They are young erythrocytes that have just expelled the nucleus: they contain an aggregate of cellular organelles, in the form of a network (hence the name) that can be distinguished only after staining with leukocytes or with brilliant cresyl blue or methylene blue.

Brilliant cresyl blue, which is a supravital dye (performed on fresh, freshly obtained cells in order to make an observation of the stained structures with live cells), stains residual RNA, Ribosomes and Mitochondria precipitated in immature erythrocytes.
Flow cytometer
Count 1000 erythrocytes
Corrected reticulocyte index
Anemias are classified according to the characteristics of the erythrocytes and also according to the regenerative capacity at the medullary level.
The corrected reticulocyte index or reticulocyte production index (RPI) is used to determine the level of regeneration and is equal to the reticulocyte index ([Htop x %reticulocytes]/Htoi) divided by the correction fraction that is adapted to the patient’s hematocrit.

*HR Under normal conditions HR is considered to be 1 and increases by 0.5 each time the Ht decreases by 10%. Thus, the FC value would be 1 for a Ht of 45%; 1.5 for a Ht of 35%, 2 for a Ht of 25% and so on (if male). If female, the FC will be 1 for a Ht of 40%.
According to the corrected reticulocyte index, the anemias are: arregenerative (IPR<2) and regenerative (IPR > 2 – 3).
An alternative to this is to calculate the absolute reticulocyte count. The normal range is 25,000-75,000/mm3. A count greater than 100,000/mm³ is in favor of regenerative anemia.
Example:
Male patient, Ht of 20, 8% reticulocytes.
Reticulocyte index = (20 x 8) / 45 = 3,55
Now, the corrected index = 3,55 / 2,25 = 1,58
Non regenerative anemia (or hypo regenerative)
Blood cell disorders

Size alterations:
Normocytic: presence of erythrocytes of normal size and volume.
Macrocytic: presence of erythrocytes whose volume is increased; they have a size greater than 8.5um.
Microcytic: red cells of smaller size than normal, approximately 7u. Typical alteration of thalassemia and iron deficiency anemia.
Megalocytic: the maximum expression of red blood cells with a diameter greater than 11u.
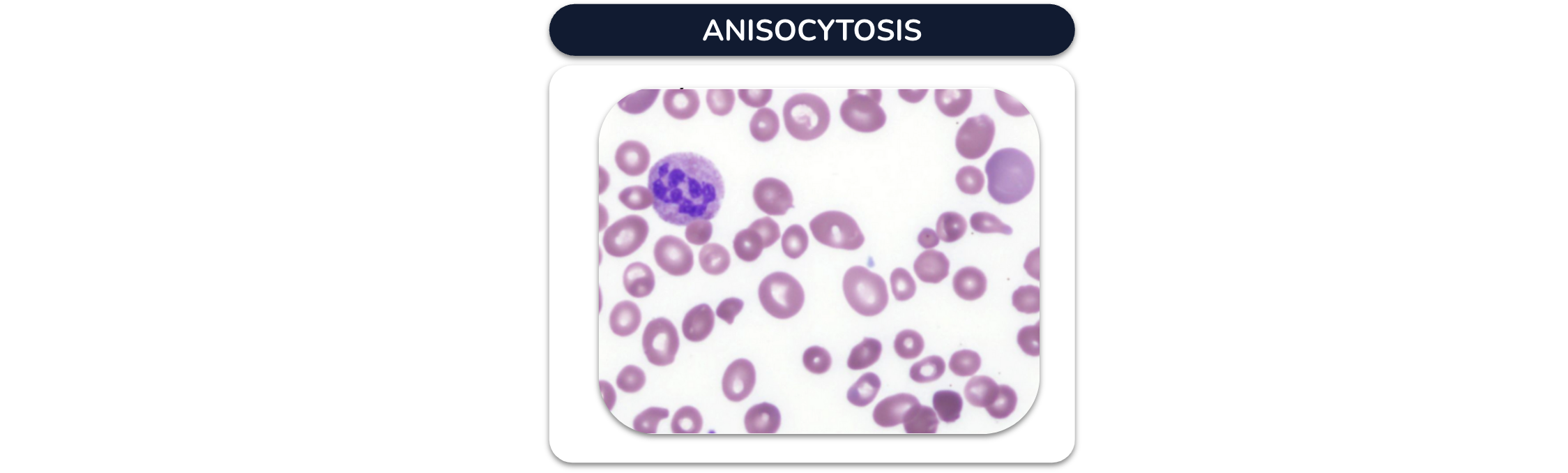
– Anisocytosis: coexistence of red cells of different sizes in the same sample. Typical of recent transfusions.
Color alterations (Hemoglobin content)
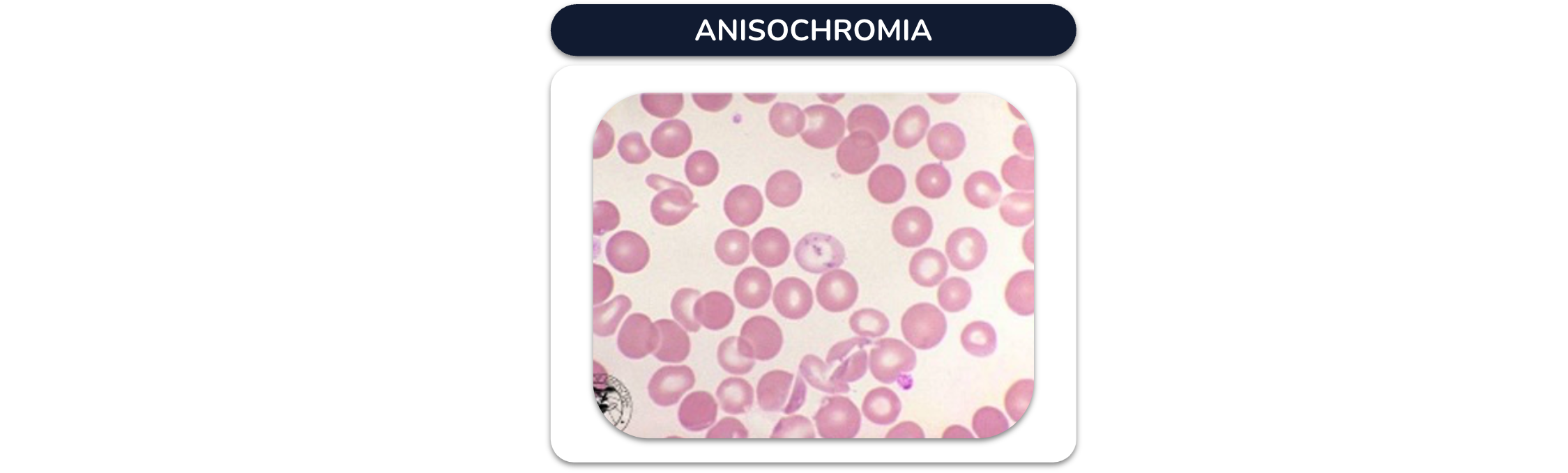
Anisochromia: Heterogeneous coloration of erythrocytes. Iron and folic acid deficiency, transfusions.
Hypochromia: the red blood cells have a lower-than-normal amount of hemoglobin. They appear pale with an evident central clarity. Decreased Hb synthesis, iron deficiency anemia, sideroblastic, thalassemia.

Hyperchromic: presence of red blood cells intensely colored due to high hemoglobin content. Hereditary spherocytosis, cell thickness alterations.

Polychromasia: reticulocytes (young red cells) showing various staining due to the presence of basophilic material in their cytoplasm. Decreased erythrocyte survival (hemolysis, hemorrhage).

ALTERATIONS IN THE SHAPE OF ERYTHROCYTES (Poikilocytosis)
Echinocyte: Serrated cell, sea urchin-like (equine), is reversible. Uremia, peptic ulcer, stomach cancer, heparin therapy, transfusions. SMEAR POORLY DONE OR NOT ALLOWED TO DRY. Crenated erythrocytes.

Acanthocyte: few spiculated projections. Alteration of lipid content in the membrane, alcoholic cirrhosis with hemolytic anemia.

Stomatocyte: Biconcave cell, mouth or stoma shape, transitional state discocyte – spherocyte, Inherited or acquired, altered Na and K permeability.

Spherocyte: hemolytic disorders, biochemical membrane lesion (spectrins).

Dianocyte or codocyte: abnormal Hb distribution. Obstructive liver disease, splenectomy, thalassemia (abnormal Hb chains), abnormal Hb.

Ovalocyte (elliptocyte): rounded ends. Hb concentrated at both ends. Megaloblastic or microcytic anemias.

Sickle cell (sickle cell): elongated cell, pointed or spiculated ends. Counterfeit anemia (HbS), acidosis.

Dacryocyte (drop cell): pear-shaped. Megaloblastic anemias, thalassemias, myelofibrosis.

Keratocyte (bitten cell): loss of a portion of membrane. G6P deficiency, thalassemias.

Schistocyte: total erythrocyte fragmentation. Defects of small ad large vessels and structural defects of the heart.

Rouleaux formation: accumulation of erythrocytes in piles of coins. Multiple myeloma, hyperproteinemia, hemolytic anemias. BAD BLOOD DRAWING. POORLY DONE SMEAR.
Erythrocyte inclusions
Basophilic stippling: due to partial degradation of ribosomes, severe anemias, lead and heavy metal intoxication.

Heinz bodies: due to precipitation of abnormal hemoglobin. Anemias due to glucose 6 phosphate dehydrogenase deficiency.

Howell-Jolly bodies are intraerythrocyte nuclear remnants seen in the peripheral blood smear with Wright’s stain. They are purple or violet spherical granules, eccentric, in erythrocytes and reticulocytes. Spleen removal, hemolytic and megaloblastic anemias.

Cabot rings: high histone content, chromatic spindles formed in mitosis. Megaloblastic anemias, lead poisoning and leukemias.

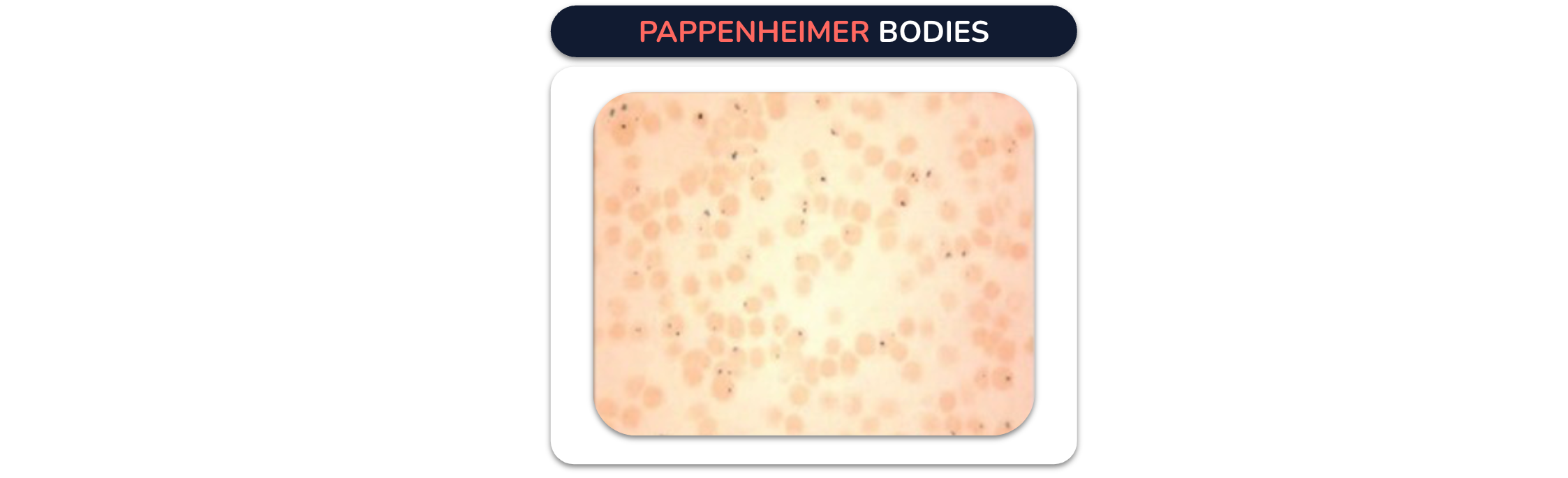
Pappenheimer bodies: secondary lysosomes of variable iron and protein composition or mitochondria with iron micelles. Siderocytes, alterations in hemoglobin synthesis (thalassemias), lead poisoning.
Platelet disorders
Platelet anisocytosis
Presence of platelets of different sizes. Larger than 5um or giant, similar to the size of a lymphocyte (immature).
Small: aging.
Mean Platelet Volume (MPV)
Measure describing the average size of platelets in the blood.
High: myeloproliferative disorders, splenectomy, etc.
Low: hypersplenism, post chemotherapy, aplastic anemia, etc.

Platelet aggregation
Disorders in platelet aggregation or adhesion processes or due to difficulty in sample collection.

Frequent alterations of neutrophils
Increase in the proportion of band neutrophils (50% or more). In infectious processes the bone marrow is stimulated and sends to peripheral blood the most mature cells, exhausting them; later it sends the cells that continue in their maturation process, the bands.

Polysegmented neutrophils, larger than normal neutrophils with hypersegmentation of the nucleus (5 or more lobules). Vitamin B12 or folic acid deficiency, chronic, myeloproliferative diseases.

Pelger-Huet anomaly
Hereditary, autosomal dominant. Incomplete lobulations of the nucleus of neutrophils and eosinophils: bilobed nucleus and scarce chromatin. Defects in chemotaxis.
Pseudo Pelger-Huet
Acquired abnormality, appears in infections, chronic myeloid leukemias, limited segmentation of neutrophils.

Toxic granulations
Larger than normal neutrophil granules, staining darker in color. Severe infections or intoxications.
They are dense lysosomes with high content of peroxidases, alkaline phosphatase and acid phosphatase. These abnormally staining azurophilic granules may lyse, which is morphologically evident as cytoplasmic vacuolization.

Auer bodies
Elongated or rod-shaped azurophilic granules found in the cytoplasm of myeloblasts and contain peroxidase and other enzymes; abnormal result of nonspecific granules. It is a diagnostic indicator for the differentiation of myeloid leukemias.

Conclusion
The complete blood cell count (CBC) comprises the study of the erythrocytes, leukocytes and platelets.
The pre analytical stage Is Important to consider because the errors occurred are critical to ensure the reliability of the results.
The CBC can be performed by manual and automated methods. There are different blood cells alterations.