
Megaloblastic anemia
Introduction
Hello, welcome to this 7th class of the Hematology course provided by the University of Guanajuato. In this class we are going to the study some basics concepts of megaloblastic anemia. Megaloblastic anemias are often the result of vitamin B12 and folate deficiencies. Ineffective hematopoiesis affects all cell lines, particularly erythrocytes. Diagnosis is based on complete blood cell count (CBC), and a peripheral blood smear that shows macrocytic erythrocytes with anisocytosis and poikilocytosis, large oval red blood cells (macroovalocytes), hypersegmented neutrophils, and reticulocytopenia. When chronic, other alterations can be observed, especially with vitamin B12 deficiency, as neurological manifestations. Treatment consists in the administration of the deficient vitamin until the symptomatology disappear.
Content development
Megaloblastic anemia comprises alterations due to nutritional deficiencies, especially vitamin B12 and folate. These vitamins are involved in DNA synthesis and regulate the differentiation of hematopoietic cells. Erythrocytes are the first cells affected, with several alterations observed: macrocytic cells with a mean corpuscular volume> 100 fL, ovalocytes, dacrocytes, inclusion bodies (Howell-Jolly and Cabot rings). Ineffective hematopoiesis affects all cell lines.

Howell-Jolly bodies: Howell-Jolly bodies are intraerythrocytic nuclear remnants that are observed in peripheral blood smear with Wright’s stain. Spherical purple or violet granules, eccentric, in erythrocytes and reticulocytes. During their maturation in the bone marrow, the erythrocytes expel the nucleus, but a small amount of DNA remains inside in some cases.
Neutrophils are particularly affected; they are observed with hyper segmented nuclei, it is considered to be a sign of megaloblastosis.

Platelet count: it is not usually altered, but there may be severe thrombocytopenia.
Macrocytosis can be due to megaloblasts or other enlarged red blood cells.
Megaloblasts are large precursors of nucleated erythrocytes with uncondensed chromatin.
Megaloblastosis precedes macrocytic anemia.
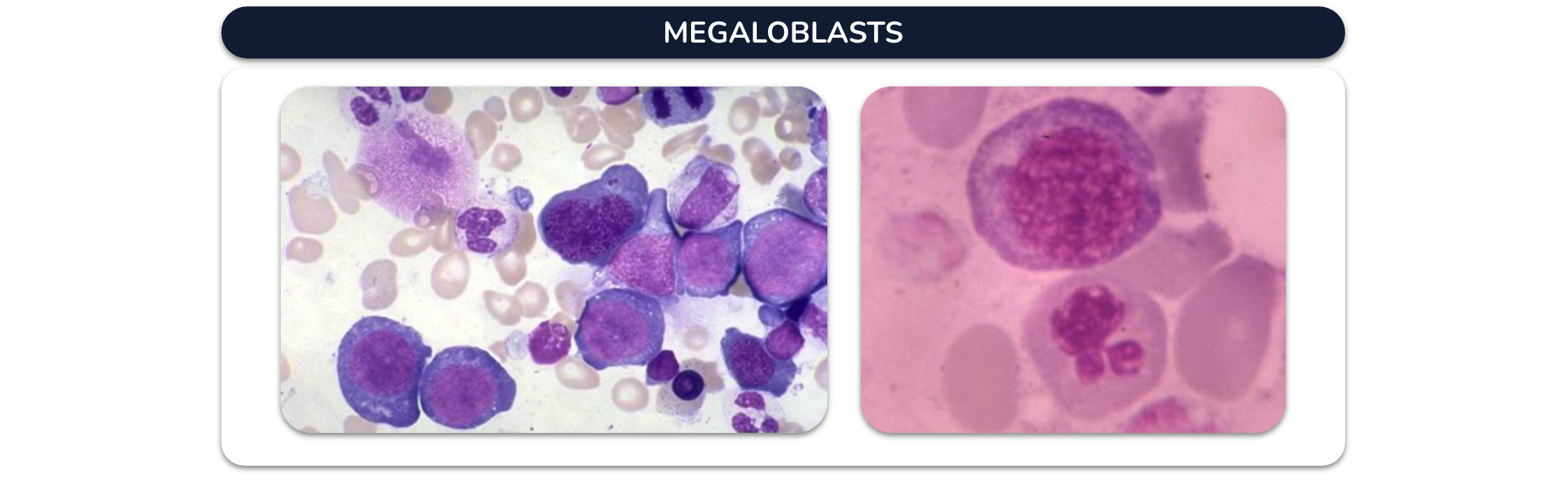
Megaloblasts
They are giant nucleated cells with nucleocytoplasmic asynchrony (abundant and hemoglobinized cytoplasm coexists with an immature nucleus), resulting from abnormal erythrocyte maturation.
Morphologically they are large cells with a mature cytoplasm, abundant mitosis, and a larger nucleus with a perforated appearance, analogous to the cut of a «sausage» or «cartwheel.»
These cells are pathognomonic of megaloblastic anemia, where 95% are secondary to a deficiency of vitamin B12 or folic acid.
Pathophysiology
The cause of megaloblastic anemia due to a deficiency of maturation factors is due to alterations in DNA synthesis.
The DNA repair mechanism, unable to cope with the excess of alterations, is fragmented and conditions premature cell death (apoptosis). This disorder has a characteristic morphological repercussion: megaloblastosis.

Normal hematopoiesis: cells most of the time, in the resting phase (G0). When mitosis (S) begins, they rapidly double their DNA content, divide, and each cell returns to the resting phase.
Megaloblastic hematopoiesis: lengthening of the S phase: there are always many more cells trying to duplicate their DNA content than in the resting phase.
They show a cell size greater than normal and finely cross-linked chromatin, typical of nuclear maturation delay (megaloblastosis, pearly chromatin).

Hemoglobin: acts as a mitotic brake, and the cell ceases its divisions, in which the cytoplasm continues to mature, the nucleus becomes pyknotic and is expelled, originating a normal erythrocyte.
In the megaloblastic line, there is a maturational nucleus/cytoplasm asynchrony, expression of abnormal DNA synthesis, which results in the cytoplasmic hemoglobin threshold occurring when few mitotic divisions have happened with the consequent mitotic brake when that cell is considerable and at pyknotize and expels the nucleus, a large red blood cell comes out into the peripheral blood.

Non-megaloblastic macrocytosis
Macrocytosis is not usually accompanied by anemia and is secondary to chronic alcoholism, chronic liver disease, hypothyroidism, and other less common causes.
Both forms of macrocytosis (megaloblastic and non-megaloblastic) can be differentiated by the morphological appearance of the macrocytes.
In megaloblastic macrocytosis the macrocytes are oval (macro ovalocytotic) and with generally very high MCV values (MCV> 110 fL), in non-megaloblastic macrocytosis the macrocytes have a normal shape (normocytes) and the MCV value is only slightly higher than 100 fL.
Pathophysiological mechanism of megaloblastic anemia:
- Erythropoiesis ineffective
- Hemolysis
Megaloblastic macrocytosis is practically always due to a deficiency of some of the essential vitamin factors for DNA synthesis (cobalamin and folate) and, therefore, constitutes a form of deficiency anemia.
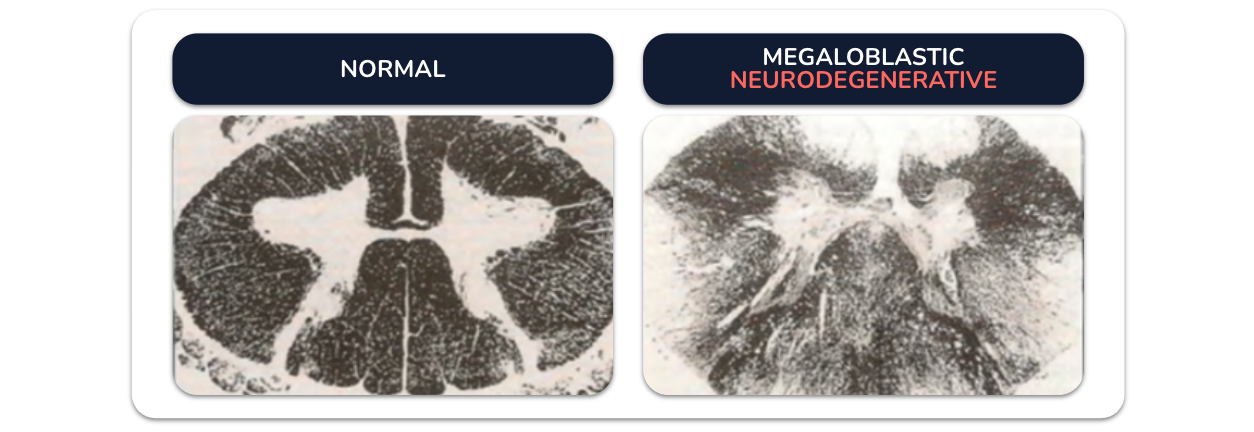
Neurological disorders due to demyelination of the lateral and posterior cords of the spinal cord.




Cbl, once released from food, binds to a transporter called haptocorrin (HC).
In the duodenum, the alkalinization of the medium and the action of pancreatic proteases (chymotrypsin, trypsin, and elastase) degrades HC, which loses its affinity for Cbl, and this binds to intrinsic Factor (Fl), which is essential for its absorption.
Cbl is transported by plasma but never circulates freely but always bound to two types of circulating proteins:
Transcobalamin II (TC-II), the natural transporter, and cobalophyllins bind Cbl, but do not transport it.

Folates and FA are absorbed in the duodenum and jejunum.
Polyglutamates are hydrolyzed to monoglutamates by the glutamate-carboxypeptidase II enzyme of the striated border.
AF is a monoglutamic molecule.
Both micronutrients share the same absorption pathway (active, saturable, and pH-dependent transport mechanism).
Absorption is mediated by two proteins expressed in the apical membrane of the enterocyte: the reduced folate transporter (hRFC) operating at neutral pH; and the acid pH-dependent proton-coupled folate transporter (hPCFT).





Clinical manifestations
General character.
Increased MCV
The patient’s age, sex, and eating habits are of great importance to carry out the diagnostic orientation since, in children, young individuals, and pregnant women, the most probable cause is folate deficiency.
Malnourished elderly, chronic alcoholics or patients with disorders of liver function (cirrhosis), intestinal absorption and metabolic diseases (hyperthyroidism) or consumptive (neoplasms).
Possible intake of medications capable of decreasing the absorption of folate.
When megaloblastic anemia appears in patients over 40 years of age, the most likely diagnosis is pernicious anemia without eating or other problems.
Penicious anemia
Megaloblastic anemia that appears in the course of atrophic gastritis is known as pernicious anemia (intrinsic factor deficiency)
Atrophic gastritis is a multifactorial disease, although with a well-demonstrated autoimmune basis and an individual genetic predisposition.
Its most outstanding characteristic is the inflammation and subsequent atrophy of the gastric mucosa (body and antrum), whose progression is carried out in three fundamental stages: superficial gastritis, atrophic gastritis, and gastric atrophy.
Megaloblastic anemia is usually the only clinical manifestation.

Biochemical tests in serum or urine
Increased concentration of unconjugated bilirubin (indirect or free) and serum lactate dehydrogenase (LDH) (Hemolysis). The deficiency of cobalamin and folate is accompanied by a characteristic increase in plasma or serum homocysteine (HCY), and urinary, whose sensitivity to detect subclinical decreases in folate and Cbl is higher than the quantification of vitamins in plasma or serum.

Treatment
2. Cbl should always be administered parenterally.
3. Isolated homocysteinemia should always be treated, even in the absence of anemia or macrocytosis.
4. The therapeutic regimen must be adjusted to the concentration of the deficient vitamin and, if necessary, implement a replacement maintenance treatment, with control being carried out every six months or every year. 5. The treatment must persist until the disappearance of the clinical or biological manifestations of the deficit.
Conclusion
Megaloblastic anemia is due to vitamin B12 and folate deficiency. It Is characterized with macrocytic erythrocytes and poly segmented neutrophils.
Homocysteine Is a metabolite that can be measured in order to detect this anemia.
It is important to determine the deficient vitamin because vitamin B12 can cause neurologic alterations. Treatment consists in the administration of the deficient vitamin.